
 One of the most common non-surgical treatments for opening obstructed coronary arteries is called Percutanueous Transluminal Coronary Angioplasty (PTCA).
One of the most common non-surgical treatments for opening obstructed coronary arteries is called Percutanueous Transluminal Coronary Angioplasty (PTCA).
Whereas twenty years ago, the majority of patients with arterial blockages were sent for bypass surgery, today many patients are now eligible for Coronary Angioplasty, a procedure that is far less invasive and requires for the majority of patients, a vastly shorter recovery time. There will still be instances where patients are referred for surgery.
Preparing for the Procedure – What do you need to do?
You should not eat or drink anything for four hours prior to the procedure. You will be given special instructions if you are diabetic. Your groin area will be washed and shaved in preparation for the PTCA. If you have had coronary angiography prior to the angioplasty, this will have been completed already.
Angioplasty Procedure – What happens?
The length of time of each procedure depends on the complexity of the individual diagnosis and situation. Procedures last between 1-3 hours for most patients. Of course, due to the nature of the procedure, each individual will encounter different parameters. Variables include the extent and nature of each blockage, as well as the number of blockages.
You will receive various medications through an intravenous line in your arm. As with angiography, you be drowsy during the procedure. The doctor may want to give you directions during the procedure.
- As with Cardiac Catheterisation, you will be placed on an x-ray table upon your arrival in the lab. Surgical sheets will cover you. Your groin will be cleansed with antiseptic and numbed. (You will feel the sting of the needle, but then your groin will feel quite numb.)
- Heart monitoring equipment will be placed on your arms and legs, and you may be given oxygen to breathe.
- The angioplasty catheter (balloon-tipped) is inserted at the numb area, and advanced to your heart, using x-ray guidance. Your cardiologist will inflate the tiny balloon in the area where the blockage occurs. It is normal when the balloon is inflated at the point of the blockage to feel chest pressure, or discomfort. Once the balloon is deflated, this will subside. Some patients feel a stronger thumping of the heart or skipping of beats. Some also feel a flushed feeling. All these sensations are normal. You will be asked at times to hold your breath for a few seconds. You may also be asked to cough.
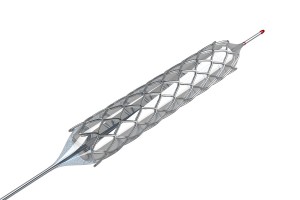
- The cardiologist may also put stents (tiny tubular shaped mesh devices that hold the arteries open) in to the arteries to inhibit the reforming of the narrowing. Newer drug eluting stents offer even greater assurance of the longevity of the repair.
- This procedure may be repeated several times if there is more than one narrowing or a narrowing that is particularly long.
After the Procedure
At the end of the procedure, a closure device for the groin incision may be used.
You will be moved to a recovery area for a short time, and then taken to your room. Your vital signs and general well-being will be monitored in the room. Your groin area and dressing will be frequently checked and you will remain in bed and keep your leg immobilised. Pain medication will be given as required and you will be required to take other postoperative medication.
You will be able to eat as soon as you wish after the procedure.
Discharge
You will be required to stay in hospital at least overnight. Your cardiologist will discuss your individual requirements with you prior to discharge.
Your cardiologist will see you the morning of discharge and discuss any further needs including follow-up consultations in the rooms and also medication. The hospital staff may also discuss these requirements with you after this consultation. You will receive prescriptions for the medicines you will need.
Possible Complications And Risk
No invasive procedure occurs without a certain amount of potential risk and complications. Your doctor and the hospital staff follow your recovery closely so that if any complications arise, corrective action can be taken immediately. Although the incidence is low, you should be aware that the following complications may rarely occur:
- Allergic reaction to the dye or to other medications.
- A tear in the artery during the procedure.
- Severe bruising/bleeding into the groin area of the procedure leg. This may come to the surface over the next few days.
- Changes in heart rhythm.
- Blood clotting
- A heart attack or stroke
‘Any surgical or invasive procedure carries risks. Before proceeding, you should seek a second opinion from an appropriately qualified health practitioner.’
Follow-up Care
Periodic follow-ups with your cardiologist are quite important. Your cardiologist will discuss when your next appointment should be made. After this, there will be a schedule of follow-ups and at least yearly consultations. In some patients, re-narrowing of the artery may occur in the future.
It is important to realise that angioplasty and stenting, whilst removing the immediate problem, do not cure coronary artery disease. It is vital that you maintain both your health and have regular visits with your cardiologist and your GP to ensure continued health. Be aware of the signs and symptoms of reoccurring heart problems and take measures to seek medical help immediately.
It is also vital to ensure that any medications you are prescribed are taken as prescribed. In patients who have had stents, there is a life-long commitment to medication.
